

Introduction
Lipoedema is a common adipose tissue disease that affects about 11% of adult women worldwide (Buck and Herbst 2016). It results from abnormal subcutaneous fat deposition with associated oedema, affecting some body parts such as the buttocks, lower extremities, and arms (Harwood et al. 1996). The cause is unknown, but it is suggested that female hormones play an important role in lipoedema formation (Reich-Schupke et al. 2017). There are currently four reported stages of lipoedema: stage 1 involves a uniform skin surface with an enlarged hypodermis; stage 2 involves an irregular skin pattern with the development of a nodular or mass-like appearance of subcutaneous fat, lipomas and/or angiolipomas; stage 3 involves large nodular fat growths that cause severe contour deformities of the thighs and around the knee, and stage 4 involves the presence of lipolymphedema (Herbst et al. 2021). One of the characteristics of lipoedema is the painful manifestation, which is accentuated by the evolution of the stage of the pathology, reducing the quality of life of women who have it. There is difficulty in treating this pathology because there is a constant inflammatory process besides the uneven fat deposition. Some surgical alternatives have been developed; however, the clinical approaches still need a scientific basis and observation of the significant results (Buck and Herbst 2016; Reich-Schupke et al. 2017; Herbst et al. 2021).
Lymphatic decongestive therapy (LLD) is the standard of care for lipoedema. It includes manual lymphatic drainage (DLM), limb wrapping, compression garments, movement therapy, dietary recommendations, and skin care. TDL has been shown to improve skin elasticity, restore the veno-arterial reflex, increase pre-lymphatic drainage and lymphatic transport in lymphatic vessels, and reduce capillary fragility in lipoedema. Intermittent pneumatic compression may not improve limb size over DLM alone but may be effective only when DLM is unavailable. Compression is most effective when tissue oedema is present. In the absence, this therapy has little effect (Kruppa et al. 2020; Shin et al. 2011).
It is suggested that shockwave therapy works similarly to lymphatic decongestive therapy in reducing oxidative stress to the tissues and smoothing the dermis and hypodermis, which may be useful as part of a treatment plan and when the lymphatics are still functioning (Goldberg et al. 2019). Another therapeutic resource that can be employed in the treatment of lipoedema is deep oscillation therapy, which uses a combination of pulsed electrostatic attraction and friction to produce oscillations that act deeply on the body's tissues, from the epidermis through the connective and adipose layers to the muscles (Boisnic and Branchet 2013). It is suggested that the physiological effects observed with this technology include reabsorption of oedema, stimulation of the wound healing process, and strengthening of skin tissues. The therapy also limits the production of inflammatory mediators, especially during the treatment of chronic pain (Boisnic and Branchet 2013; Buchan 1971).
Since it is a condition that involves different components in its treatment, it is necessary to search for technologies that can be associated with a more efficient therapy. However, there was a scarcity of studies on shock wave therapy and deep oscillation therapy in the treatment of lipoedema, besides being unknown the possible benefits of this association. Therefore, this study aims to investigate the effects of shock waves and deep oscillation on lipoedema by evaluating their results individually and together and establishing a protocol to be used.
Methodology
This is an experimental study. For the study, 33 female volunteers who met the following inclusion criteria participated: women between 20–50 years of age, body mass index (BMI) indicating grade II obesity, not suffering from diabetes, or with a history of kidney problems, who were not pregnant or in a postpartum period of up to 12 months, or who were undergoing any treatment or hormone therapy, or who had neoplasms. Volunteers would be excluded in case of dropout or complications from adverse responses after the procedures.

The research was submitted to the Plataforma Brasil and approved by the ethics in research committee of the Universidade Potiguar - UnP, Natal/RN, with opinion 5.265.850. The participants were not subject to any dietary restriction and were asked to maintain their daily activities in a usual manner. After being informed about the study's objective and the procedures that would be used, the participants signed the informed consent form.
Then, an evaluation form was submitted with general information about each volunteer. In the evaluation of the volunteers, ultrasonography was also performed in an ultrasound scanner (SonoScape S9, China) of the malleolar region at the knee.
The perimetry was performed using a fibre metric tape that measures the circumference 5 cm below the umbilical scar. Later, the measurement was performed on the iliac crest bilaterally for the hip, serving as a reference point for the subsequent measurements of the lower limbs, performed every 10 cm in every lower limb. Subsequently, the total measurement of each limb was made. The treated limb was standardised on the right side for all groups, while the left limb was kept as a control.
Then the evaluation was performed using a bioimpedance scale (Equipo Omron model HBF514C), where the composition and distribution of the percentage of fat (% fat), percentage of visceral fat (% visceral fat), body mass index (BMI), percentage of muscle mass (% muscle mass) and body age were observed.
For the treatment, the volunteers were divided into three equal groups: G1 received the treatment with deep oscillation, G2 with shockwaves (OC), and G3 received the treatment with the two associated techniques, shockwaves associated with deep oscillations (OC+ deep oscillations). The duration of treatment was five sessions, being performed once a week.
The treatment was carried out using a shockwave device (Radial Shock waves, Dolor Clast equipment, Electro Medical Systems, Switzerland), with the following parameters for shockwaves: between 1, 8 and 2, 5 Bar; 12 Hz; 500 pulses in the ankle area; 500 pulses in the internal area of the knee (upper third); 500 pulses in the inner part of the thigh. For deep oscillation (Deep oscillation equipment, Physiomed, Germany), we used between 150 and 70 Hz for 3 minutes; 30 to 10 Hz for 4 minutes; and between 75 and 50 Hz for 3 minutes, a total of 10 minutes on a single limb.
The re-evaluation was done after the last treatment. The volunteers were re-evaluated using the same methodology employed pre-treatment.
The volunteers were seen at the Dermato functional physiotherapy treatment clinic at the International Oncotherapies Institute, Santiago, Chile.
The collected data were organised in Excel tables, and quantitative data were submitted to statistical analysis. Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) software version 22.0 for Windows. First, the Kolmogorov-Smirnov (K-S) test was performed to verify the normality of the data. In the inferential statistics, we used the two-way ANOVA test with repeated measures to verify differences between the groups before and after the interventions. A 5% significance level and 95% confidence interval (95% CI) were assigned in all statistical analyses. Qualitative data (descriptive analysis of the ultrasound images) were described based on the medical reports.
Results
Table 1 presents the results of the anthropometric and bioimpedance values observed in each research group, comparing the means of each group between the time of the initial and final evaluation and between the OC, deep oscillation, and OC + deep oscillation groups.
Table 1. Comparative analysis of anthropometric and bioimpedance variables between the groups and between the initial and final moments
| BMI | Initial | Final | P value |
|---|---|---|---|
| OC | 24.72±3.73 | 24.55±3.82 | 0.99 |
| Deep Oscillations | 29.4±3.02 | 29.32±2.97 | 0.98 |
| OC+ Deep Oscillations | 26.5±3.95 | 26.14±4.02 | 0.99 |
| p-value | 0.87 | 0.83 | |
| %Fat | |||
| OC | 47.67±6.57 | 47.04±5.43 | 0.99 |
| Deep Oscillations | 46.7±7.48 | 43.02±4.19 | 0.73 |
| OC+ Deep Oscillations | 46.15±4.56 | 34.54±5.55 | 0.04* |
| p value | 0.98 | 0.97 | |
| %Muscle Mass | |||
| OC | 24.07±4.21 | 25.07±1.51 | 0.96 |
| Deep Oscillations | 23.12±2.38 | 22.5±1.27 | 0.96 |
| OC+ Deep Oscillations | 24.81±3.08 | 25.32±2.9 | 0.94 |
| p value | 0.96 | 0.83 |
Note: *Significant difference with p < 0.05.
Table 1- Comparative analysis of anthropometric and bioimpedance variables between the groups and between the initial and final moments.
No significant difference was detected in the comparative analysis of anthropometric and bioimpedance variables, only in the OC + deep oscillations group in the % fat variable compared to the initial and final time (p=0.04).
Table 2 presents the graphic results of the table. It can be observed that the OC + deep oscillations group presents a more significant reduction in perimetry measurements, probably characterising a reduction in oedema with the analysis of the initial and final moments.
Table 2. Comparative perimetry analysis between the control side (CEM) and the treated side (TDM)
| Initial Moment | Control (MIE) | Treated (MID) | p value |
|---|---|---|---|
| Control × OC | 18.44±1.12 | 18.22±1.21 | 0.87 |
| Control × Deep Oscillations | 18.99±1.45 | 18.11±1.1 | 0.89 |
| Control × OC+ Deep Oscillations | 18.1±1.1 | 18.32±0.9 | 0.92 |
| p value | 0.96 | 0.94 | |
| Final Moment | Control (MIE) | Treated (MID) | P value |
| Control × OC | 17.54±1.1 | 14.21±1.2 | 0.04* |
| Control × Deep Oscillations | 17.32±1 | 13.32±1.3 | 0.02* |
| Control × OC+ Deep Oscillations | 15.98±1.3 | 10.21±1.1 | 0.001* |
| p value | 0.67 | 0.04* |
Key: Control (MIE): There was no statistically significant difference. Treated (MID): There was a significant difference in the comparisons Control × OC:0.04; Control × Oscillations: 0.02 and Control × OC+ deep oscillations: p=0.001.
When the analysis was carried out comparing the control and treated sides, it was observed that there was no difference in perimetry at the initial moment. The final comparison showed a significant reduction in the perimetry of the treated side compared to the control side in all groups, respectively, control × OC (p=0.04), control x deep oscillations (p=0.02) and control × OC+ deep oscillations (p=0.001).
Table 3 shows the ultrasound results of the epidermis, dermis, and hypodermis layers.
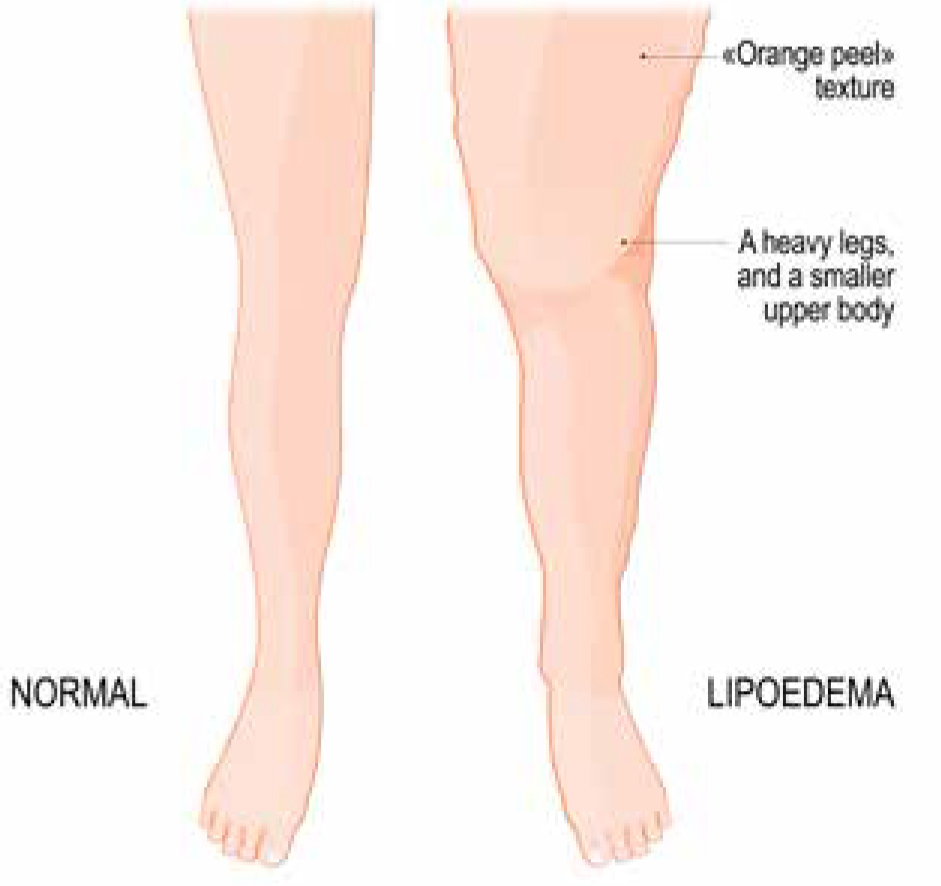
Table 3. Analysis of the ultrasound of the lipoedema region in the layers of the epidermis, dermis, and hypodermis.
| Epidermis | Initial Control | Final Control | p value | Initial Treaty | Final Treaty | p value |
|---|---|---|---|---|---|---|
| OC | 0.8±0.09 | 0.7±0.02 | 0.95 | 0.6±0.09 | 0.5±0.02 | 0.91 |
| Deep Oscillations | 0.6±0.01 | 0.5±0.07 | 0.92 | 0.5±0.01 | 0.4±0.07 | 0.94 |
| OC+ Deep Oscillations | 0.5±0.08 | 0.55±0.07 | 0.99 | 0.5±0.08 | 0.35±0.07 | 0.9 |
| p value | 0.89 | 0.87 | 0.9 | 0.9 | ||
| Dermis | ||||||
| OC | 1.6±0.09 | 1.4±0.05 | 0.78 | 1.6±0.09 | 1.4±0.05 | 0.05 |
| Deep Oscillations | 1.5±0.01 | 1.3±0.09 | 0.83 | 1.5±0.01 | 1.3±0.09 | 0.09 |
| OC+ Deep Oscillations | 1.7±0.08 | 1.6±0.07 | 0.91 | 1.7±0.08 | 1.4±0.07 | 0.07 |
| p value | 0.9 | 0.9 | 0.9 | 0.9 | ||
| Hypodermis | 0.98 | 0.95 | ||||
| OC | 1.6±0.08 | 1.5±0.15 | 0.99 | 1.6±0.08 | 1.4±0.15 | 0.89 |
| Deep Oscillations | 1.8±0.07 | 1.7±0.06 | 0.98 | 1.8±0.07 | 1.6±0.06 | 0.91 |
| OC+ Deep Oscillations | 1.7±0.05 | 1.8±0.06 | 0.96 | 1.7±0.05 | 1±0.06 | 0.03* |
| p value | 0.98 | 0.96 | 0.91 | 0.04+ |
Legend: *showed a statistically significant difference compared to the initial moment p=0.03.+ showed a statistically significant difference with lower volume in the OC + deep oscillations group compared to the other groups p= 0.04.

A reduction in the hypodermis can be observed in the group that performed OC + deep oscillations when comparing the initial and final time points (p=0.03) and when comparing with the other groups (p=0.04).
Table 4 compares the perimetry between the control and treated side in the perimetry analysis.
Table 4. Comparative perimetry analysis between the control side (CEM) and the treated side (TDM)
| Final Moment | P value |
|---|---|
| Epidermis | |
| Control × OC | 0.43 |
| Control vs. Deep oscillations | 0.21 |
| Control × OC+ oscillations Deep | 0.15 |
| Dermis | |
| OC | 0.56 |
| Deep Oscillations | 0.25 |
| OC+ Deep Oscillations | 0.45 |
| Hypodermis | |
| OC | 0.12 |
| Deep Oscillations | 0.21 |
| OC+ Deep Oscillations | 0.03* |
Key: Control (MIE): There was no statistically significant difference.
Treated (MID): There was a substantial difference in the comparisons control × OC: 0.04; control × oscillations: 0.02 and control × OC+ deep oscillations: p=0.001.
It can be observed that the OC + deep oscillations group presented a reduction of the hypodermic layer by ultrasound in comparison with the initial moment and with the other groups, demonstrating the possibility of an effective action on the fat layer in the area of the lipoedema when the association of treatments was used. In the comparison between the control and treated side, a reduction in the control group × OC+ deep oscillations can be observed (p=0.03).
The figures below show the images of each group between the initial and final moments.
The OC+ deep oscillations combination therapy group has a visually better clinical outcome, observed qualitatively in the figures below.
Discussion
The present study evaluated the effect of combined shockwave therapy associated with deep oscillation and their isolated modalities in treating lipoedema. In the anthropometric analysis, it can be observed that all forms of application presented similar behaviour without significant change. Only the variable fat percentage showed a reduction in the group OC + deep oscillation compared to the initial and final moments. Also, the groups' deep oscillation and shock waves analysed separately. In the perimetry analysis, the OC + deep oscillation group presented a significant reduction in its measurements compared to the initial moment and the other groups.
The combined shockwave therapy and deep oscillation showed an efficient response in treating lipoedema with reduced body fat percentage. Shockwave therapy promotes the reduction of localised adiposity and the improvement of blood and lymph flow (Goertz et al. 2012; Modena et al. 2017). Shockwaves positively affect angiogenesis and leukocyte behaviour and increase blood flow (Goertz et al. 2012; de Lima Morais et al. 2019). In other dysfunction models, as in cellulite and localised adiposity, shock waves favour a reduction in fat concentration, improved local circulation, and functional tissue improvement. According to the findings of this study, in lipoedema, shock waves used alone did not promote a significant reduction in body fat percentage. Still, when combined with deep oscillations, this result was effective (Maia R et al. 2020; Zapata et al. 2021; Ferraro et al. 2011).
It can be observed that the combination of OC + deep oscillation promoted a reduction of the hypodermis layer on ultrasound. This result can be justified by the action that shock waves produce rupture of the adipose tissue membrane through unstable cavitation generated (Chen and Liang 2008). Through the observation of adipose tissue slides in animals, it was verified that the adipose tissue is damaged by two types of mechanisms: compression and cavitation (Liang 2008). It is believed that the effect of compression pressure causes a modification with rupture of the fat cells and that the cavitation effect causes an irregularity and, consequently, lipolysis (Chen and Liang 2008; Liang 2008). It is suggested in this study that the use of deep oscillations enhances the action of shock waves, contributing to tissue reorganisation.
In lipoedema, the reduction of adipose tissue may be a significant component of tissue remodelling. However, this response was accentuated only in the group associated with deep oscillation, suggesting that it promotes a greater circulation of inflammatory and interstitial fluid (Kraft et al. 2013; Aliyev 2009). A mechanism of deep oscillation with electrostatic waves promotes smooth vibrations in the tissues and electrolytes, observing the lymphatic and circulatory activation, thus reducing the fluid concentration between the fat cells (Aliyev 2009), (Fistetto et al. 2011; von Stengel et al. 2018).
The combination of the two forms of intervention can provide even more significant benefits in the treatment of lipoedema, observed through reduced perimetry in both limbs tested. Combined shock wave therapy and lymphatic drainage may help to minimise oedema, improve lymphatic function, and relieve pain and discomfort in patients with lipoedema. Besides the physiological responses promoted, one can observe a clinical improvement in the qualitative analysis of the skin aspect, as visualised in the comparison of the figures before and after the interventions (Ferraro et al. 2011; Angehrn 2008; Christ 2008).
There is scientific evidence of improvement in lipoedema with the combined therapy, with limitations regarding histological analysis and dynamics of the lipoedema picture, suggesting that further studies should be carried out with a larger population and immunopathological analysis of the treated tissue.
Conclusion
The association of shock wave therapy with deep oscillation promoted a reduction in the perimetry of the left lower limb, with a lower percentage of fat and a visible qualitative improvement in the aspect of lipoedema when compared to the initial moment and to the groups that did only one of the interventions.
What is lipoedema? A reminder:Lipoedema is a common adipose tissue disease that affects about 11% of adult women worldwide. It results from abnormal subcutaneous fat deposition with associated oedema, affecting some body parts such as the buttocks, lower extremities, and arms. The cause is unknown, but it is suggested that female hormones play an important role in lipoedema formation.
CPD reflective questions
- Have you ever come across lipoedema in your practice?
- Are you familiar with the causes?
- Are you aware of the treatment options?