

 Dr Irfan Mian
Dr Irfan Mian
The neck is a difficult area to treat. There are major arteries, veins, nerves and other anatomical structures that must be avoided when performing any neck procedure. Excessive loose skin in the upper neck, also commonly known as ‘turkey neck’, is a common aesthetic problem in middle-aged males and females. Many men undergo surgical Z-plasty to correct this (Biggs and Steely, 2000). However, today, polydioxanone threads are commonly used as an alternative to surgery to improve the appearance of turkey neck.
 As one of the first areas to show ageing, the neck is a popular area for treatment. However, due to major arteries, veins and nerves, it can be difficult to treat, so a full understanding of the anatomy, as well as the procedure in question, is crucial
As one of the first areas to show ageing, the neck is a popular area for treatment. However, due to major arteries, veins and nerves, it can be difficult to treat, so a full understanding of the anatomy, as well as the procedure in question, is crucial
Thread material
While polydioxanone threads are a popular choice of thread material, other materials, such as poly-L-lactic acid, polycaprolactone silicon-covered thread, gold and others are available to be used.
The author's preferred material is polydioxanone. Crucially, this material is broken down into water and carbon dioxide, is bio-compatible and promotes neocollagenesis. Indeed, even polydioxanone filler material has a bio-stimulatory effect (Kwon, 2019).
The other materials mentioned have properties that can sometimes give rise to post-treatment complications, such as inflammatory nodules, erythema and oedema, as well as disfigurement that can be a result of the aforementioned (Storer et el, 2016).
Protocol and method
The current protocols for the treatment of neck laxity give mixed results in clinical practice. The technique involves the placement of cog threads horizontally parallel to the lower border of the mandible. To improve results, mono or twisted mono polydioxanone threads are often required.
Clinical audit results show that the neck lift achieved was moderate and there was a problem with longevity. Many cases relapsed after 6 months. The polydioxanone threads themselves were of a diameter that did not give good tensile strength, resulting in poor mechanical tension.
» This recommended technique is not for the inexperienced practitioner as it involves a detailed knowledge of the anatomy of the submental and upper neck area so that damage to structures can be avoided «
The threads themselves were of the ‘machine-cut’ variety, unlike the modern mould compressed threads. Machine-cut polydioxanone threads involve the thread being cut with a sharp blade to create pointed cogs. A wide variety of cut threads are available on the market. Cogs on the threads can vary in size and position. They can be uni-directional, bi-directional (with or without an inter-cog space) or a combination of both. Cogs can also be spatially arranged so that a 2D, 3D, 4D or 5D pattern is produced longitudinally. The cogs can be placed in line, randomly or helically. A detailed description of the reasons for the manufacture of all types of polydioxanone threads is outside the scope of this article.
 Figure 1. The patient pre-thread lift
Figure 1. The patient pre-thread lift
Overcoming the hurdles
The major problem with machine-cut threads is that, due to the relatively delicate pointed cut, there was degradation, even after 14 days. This degradation was most likely the major factor involved in tissue laxity following thread lift procedures. Furthermore, this would also compromise the longevity of the treatment.
These problems have been overcome by HansBiomed Corp, which has patented the press mould method. The threads are also bi-directional. This means that the press mould cogs point in opposite directions, which helps keep the thread from migrating as happens with uni-directional cog threads. The threads are also thicker so that tensile strength is good. The cogs on the polydiaxanone threads are arranged in a helical pattern, which results in improved vectors. These technical manufacturing changes all carry a patent.
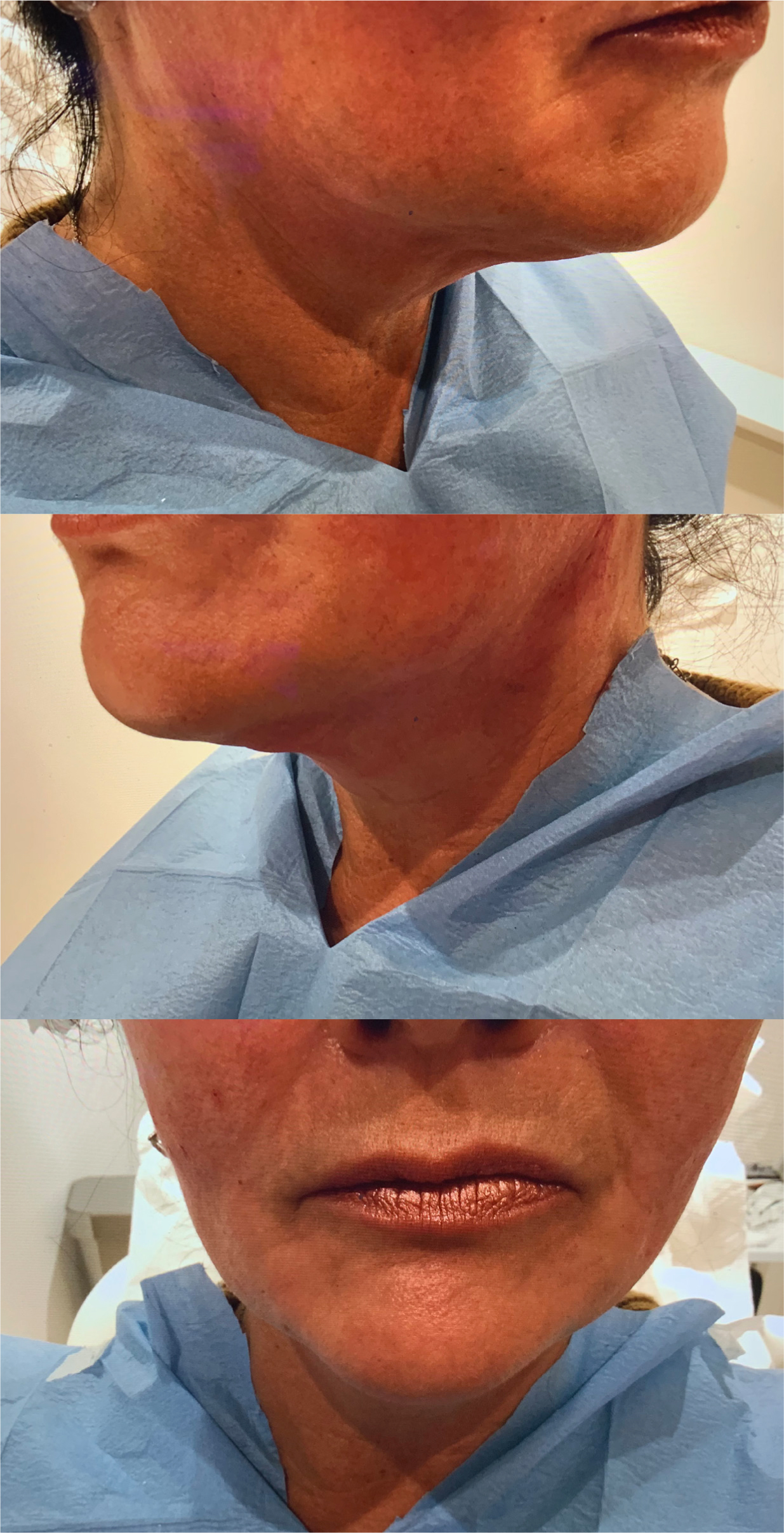 Figure 2. The patient immediately post-thread lift
Figure 2. The patient immediately post-thread lift
These improved technological advances mean that modern threads are stronger, longer lasting, and have greater tissue lifting capacity. In the hands of experienced and appropriately trained practitioners, the results are optimal and the downtime for the patient is minimal.
Despite advances in thread technology, there are still problems in getting a good aesthetic result; this was especially true in the case of submental skin laxity. Determining the X and Y vector axis lines to achieve a resultant vector direction is not easy to do. The threads have vector forces similar to the position of iron filings placed on paper over a stick shaped magnet. Allowances must be made for the variable factors, such as size of thread both diameter and length and the number of cogs and so on.
A new technique
For ease of application and achieving optimum results, the author has pioneered a new technique. This recommended technique is not for the inexperienced practitioner as it involves a detailed knowledge of the anatomy of the submental and upper neck area so that damage to structures—such as the external and anterior jugular vein, the cervical branch of the facial nerve and even the carotid artery and sinus—can be avoided.
The reason for this is that part of the treatment involves using two sharp needles attached to the polydioxanone threads. These needles are available from HansBiomed Corp and are 13 cm long, while the thread is 42.4 cm long.
These twin sharp needles are placed in parallel pairs, entering the neck from the midline and exiting at approximately 1 cm from the base of the mastoid process on each side. Care must be taken near the mastoid exit to avoid puncturing the external jugular vein. The author recommends a particular technique to avoid anatomical structures. This technique, called the ‘half wave’ needle advancement technique, must be mastered by the clinician. The threads are placed in the subplatysmal tissue and these horizontal threads enter near the skin position of the mandibular genial tubercles in the sagittal plane.
Next, the twin needles are left in situ and two vertical cogs should be inserted towards the upper border of the larynx. Their entry point is in the middle third of the ala-tragal line and these vertical threads interlink with the horizontal threads to give an excellent upward vector by pulling up the lax neck tissue. These vertical threads support the horizontal threads by crossing the jawline between the medial insertion of the masseter muscle (medial to the facial artery and notch) and the mandibular retaining ligament. It is very important to ensure that the threads placed vertically are placed deep to the horizontal threads. The number of threads used will vary according to the amount of neck lift required. On average, a total of eight threads are used.
This area of the submental region is where dissection of the medial fibres of platysma are cut in a surgical neck lift, as described by de Castro (2003). The author's technique mimics this without surgical intervention. In this way, a resultant vector in an upward and lateral direction is created, thereby lifting the neck.
In conclusion, in the hands of suitably trained clinicians the author's technique gives very good results, without the need for surgical intervention and longer periods of downtime.
 While polydioxanone threads are a popular choice, other materials such as poly-L-actic acid may be suitable for the procedure
While polydioxanone threads are a popular choice, other materials such as poly-L-actic acid may be suitable for the procedure