

Experience since the introduction of laser and intense pulsed light (IPL) treatments for long-term hair reduction has shown that almost all skin types, including European, Asian and Middle-Eastern, respond well to treatment (Johnson and Dovale, 1999; Dierickx, 2002). Varying cultural influences, including traditional factors, fashion, sport, personal feelings of wellbeing and health requirements, have dramatically increased demand around the world, from both women and men, for long-term hair reduction.
Only very dark skin types, particularly Afro-Caribbean and some South Asian skin types, are problematic because the high levels of melanin in the epidermis absorb light energy in competition with the targeted melanin or haemoglobin in the hair follicle. Ginger, blonde and grey/white hair responds poorly to light-based treatments in hair reduction.
The need for a rapid, non-invasive method to remove unwanted body and facial hair led to the use of lasers by medical practitioners in the late 1980s and to the development of professional intense pulsed broadband light devices, which first entered the US market in 1994 (Grossman et al, 1996). Since then, numerous manufacturers have developed competitive systems resulting in a dramatic price reduction. Lower prices, technological advances and a lack of regulatory controls on IPL devices have popularised their use among beauty therapists and salon owners as well as many private medical practitioners in many countries. Miniaturisation of opto-mechanical components and recognition that low-energy hair-reduction appliances were effective in achieving hair-growth delay also led to the development of simple, portable home-use devices entering the market in 2006 (Kline, 2019; Town et al, 2019).
The hair growth cycle and photoepilation
Hair in the anagen, or ‘growing’, phase is considered to be ideal for light-based hair-reduction treatment when the maximum potential exists for absorption by melanin and blood in the hair shaft and dermal papilla (Purba et al, 2014).
Although human hair grows in cycles, it is asynchronous with all stages of hair growth present at any one time. Thus, hair follicles not in the anagen phase at the time of treatment will continue to grow after treatment. Even after hair has been removed by light-based therapy, the reduction may not be obvious initially, and multiple treatments are required to match the natural hair-growth cycles (Figure 1).

The best target for light-based hair reduction with the greatest efficacy and safety from side effects is dark coarse hair with a strong contrast between hair and skin colour. Light, sandy-coloured hair on a pale skin is difficult to treat successfully, although black, coarse hair on a dark skin will respond well to laser or even IPL treatment.
Experience has shown that multiple treatments are required for hair removal. This is due to the nature of the hair growth cycle as explained above, and an average of four to eight sessions is needed for hair removal. The gap between sessions is 4–10 weeks depending on the new growth and the body area being treated. Average rates of long-term hair reduction (measured at 6 months after completion of treatments) have been reported typically in the range of 50–90% (Dierickx et al, 2002; Lepselter and Elman, 2004; Drosner and Adatto, 2005). However, there have been relatively few randomised controlled studies and none examining hair-reduction rates beyond 2 years (Haedersdal and Wulf, 2006).
It is never recommended to repeat professional treatments in under 4 weeks as the full recovery period for the skin is generally 28 days.
The initial target is the melanin in the terminal hair shaft, which converts absorbed light energy into heat that in turn is conducted by thermal perfusion throughout the entire follicle and into adjacent tissue where germ cells are located (particularly around the dermal papilla at the base of the hair bulb, in the so-called ‘bulge’ area and along the follicle). It is these germ cells that are believed to be primarily responsible for hair regrowth (Cotsarelis et al, 1990). Providing sufficient heat is generated, these cells are damaged or entirely disabled preventing the hair from regrowing. Any delayed partial regrowth may be thinner and/or lighter than the original, treated hair.
The most responsive hair to intense light or laser absorption is terminal or ‘adult’ hair, which, providing the hair has sufficient melanin (pigment) and depending on the hair's thickness, will provide a good chromophore (light absorbing target) for photothermolysis.
Skin types
It is important to identify not only the colour and thickness of the hair, but also the tone of the overlying skin as this will have a bearing on selection of the energy output of the laser or IPL that will be used. The reaction of different skin colours to ultraviolet light was developed by Thomas Fitzpatrick in 1972, which led to the broad adoption of the Fitzpatrick skin phototype reference scale (Fitzpatrick, 1988). This scale identifies six different genetic skin types, skin colour and reaction to first average sun exposure in terms of tanning or burning and is routinely used for client assessment in laser and IPL hair removal (Sachdeva, 2009).
Generally, the best results will be achieved where there is little natural melanin in the skin with a heavy concentration of melanin in the hair. This is because the amount of melanin creating the skin tone is considerably lower than the melanin in the cylindrical shaft of the hair. Thus, the hair shaft will preferentially absorb the light, which is converted into heat energy within the hair rather than in the surface layers of the skin.
Colour and thickness of the hair play a major role in the absorption process of intense pulsed light or laser light as indeed does the skin tone. Darker, thicker hair with eumelanin—brown or black pigment—will absorb the light more readily than lighter, finer hair, which will require adjustments to the energy density and pulse duration. The contrast between the colour of the hair and the skin tone is extremely important as the hair is the prime absorber, not the skin. Lower energy and longer pulse durations are employed in darker skin types to further reduce the risk of skin injury. Because of the very high melanin content in Fitzpatrick skin type 6, IPL hair reduction is contraindicated, although long-pulse near-infrared lasers such as the Nd:YAG laser at 1064 nm can be used with caution.
Pheomelanin produces yellow and ginger to red tones within the hair structure and this type of melanin does not absorb laser light or broadband IPL light very well. People with this lighter type of pigment generally have paler skin and burn easily when exposed to UV light. System parameters, including choice of wavelengths(s), pulse duration and energy density or ‘fluence’ may be optimised to give the best results according to hair type, and hair and skin colour.
Treatment parameters
Wavelength
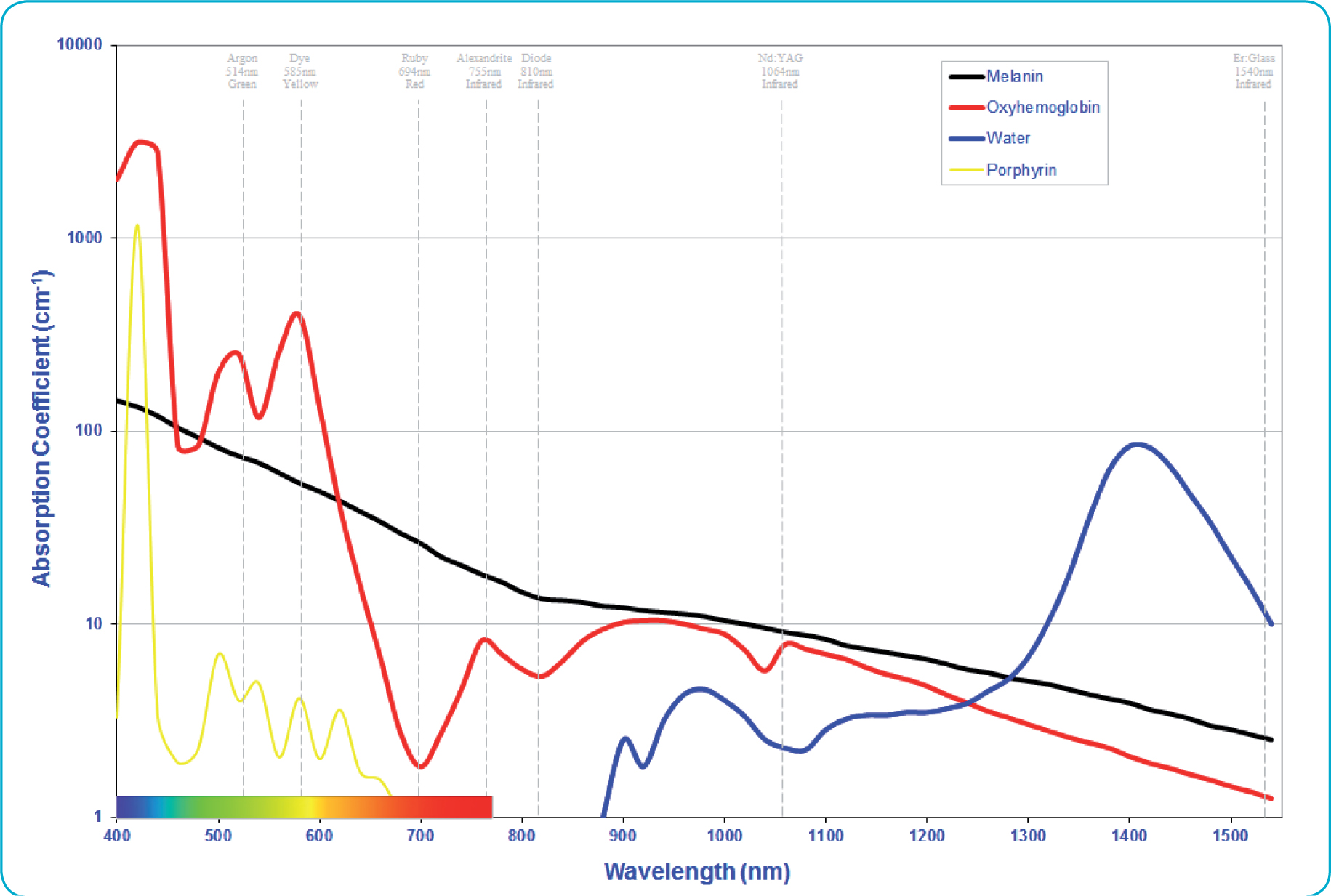
Two principles should be considered when choosing the optimal light wavelength for hair removal: scatter and absorption. Light scatters as it enters the skin. Longer wavelengths penetrate further into the skin to reach deeper-lying hair follicles. Shorter wavelengths of light scatter more readily (Anderson and Parrish, 1981; Jacques and Prahl, 1987). Therefore, it is important to select a wavelength that will reach the target in the tissue. For example, adult terminal hair follicles and their vital adnexa may extend deep into the subcutaneous layer. Blue light, with shorter wavelengths, is very well absorbed by the target melanin in the hair shaft and bulb, but is unable to reach sufficiently deeply into the skin to thermally disable the target hair follicle.
IPL devices produce mostly visible broadband wavelengths of light. Potentially harmful, short-wave UV light is filtered out by the lamp enclosure itself, and very little long-wave infrared light is produced by a xenon lamp. The remaining wavelengths, between 500 and 1000 nm, are all well absorbed by melanin and so are suitable for hair removal. Optimal wavelengths for photoepilation are between approximately 600 and 820 nm (Figure 2).
Spot size
The larger the spot size, the deeper the penetration of laser or IPL light into skin and the less that energy is lost at the edge of the treatment area (Figure 3). Some IPL devices use U-shaped or twin-flash lamps to produce a large, rectangular spot size on skin (as much as 9–12 cm2), which ensures that light energy penetrates deeper into tissue to reach the base of the hair follicle (Manstein et al, 2001).

Pulse duration
Pulse duration is another important parameter to consider. Generally, the pulse of laser or IPL light used will be longer for thicker hair and shorter for finer hair. By choosing longer pulses of light for hair removal, the operator will also reduce the risk of collateral damage to the skin as the tiny particles of melanin in the skin have time to lose absorbed heat during a long pulse (compared with a much larger hair follicle that will hold its heat longer). This process is called ‘selective photothermolysis’ (Anderson and Parrish, 1983; Altshuler et al, 2001).
The pulse of laser or IPL energy is calculated to match the ‘thermal relaxation time’ (TRT) of the hair follicle so that no significant injury is caused to skin. This is achieved due to the very short TRT of the skin compared with the hair follicle as the melanocytes (epidermal melanin-containing cells) are able to lose heat much more rapidly than the hair follicle, thus restricting thermal damage to the hair.
Selective photothermolysis, first proposed by Anderson and Parrish in 1981, involves matching of a specific wavelength of light coupled with the precise pulse duration and fluence to obtain the maximum outcome without damage to the surrounding tissue (Anderson and Parrish, 1981). It employs knowledge of the rate of heat gain and loss from specific targets, such as the melanin in hair follicles. It also uses the most effective wavelength, optimum energy density and pulse duration to precisely damage an absorbing biological target while minimising collateral damage (Anderson and Parrish, 1983).
Energy required for successful treatment of hair
There are several factors that determine choice of energy level. The overall objective is to find the optimal ‘therapeutic window’ where laser or IPL energy is sufficient to damage the hair follicle but avoid injury to surrounding tissue and consequential undesired side effects. Normally, the skin will only feel warm temporarily after treatment and any redness will disappear within minutes or a few hours.
Darker skin (including suntan or spray-tan) and greater hair density reduces the amount of possible energy you can use before side effects appear. This will vary from person to person and body area to body area.
Hair reactions to laser and IPL therapy
Photothermal effects on the targeted chromatophore result from the absorption of the laser or IPL light energy. Depending on the wavelength, this process simultaneously causes localised heating of the chromophore with the end outcome of coagulation, vaporisation, cutting, ablation, and/or destruction of the target medium. Photothermal effects account for most of types of aesthetic, surgical, medical and therapeutic laser and IPL procedures (Figure 4).

Light-based hair depilation
In the case of a terminal hair follicle, irradiative energy is scattered beneath the skin surface and absorbed selectively by the melanin-rich hair shaft and follicular matrix, and possibly by haemoglobin absorption in the blood supply to the dermal papilla. This heat is then transferred by conduction, to adjacent cells, including those around the dermal papilla at the base of the hair bulb and the so-called ‘bulge’ area in the outer root sheath located near the insertion of the erector pili muscle. The heat absorption causes the surrounding cells that cause hair regrowth to die and therefore inhibit the follicle from producing further hairs. The result is an induced change in normal hair cycling as the hair follicle moves into telogen induction (hair regrowth inhibition).
As there is also melanin in the epidermis (giving the skin its natural colour), care must be taken to select appropriate energy levels to induce the desired therapeutic outcome without damaging surrounding normal tissue. Darker skin, darker, thicker hair and greater hair density all require lower energy levels. Lighter skin, lighter thinner hair and lower hair density, all require higher energy levels. White or vellus hair is virtually unaffected by photothermal treatment.
As described previously, the process of selecting the hair follicle and its adjacent cells to damage with discrete pulses of light energy is called ‘selective photothermolysis’ and depends upon the fact that smaller bodies such as epidermal melanocytes lose heat faster than larger bodies like hair follicles. The smaller relative surface areas of melanin particles lose heat faster than the much larger hair shaft. Generally, the pulse of laser or IPL light used will be longer for thicker hair and shorter for finer hair. According to the generally accepted theory of selective photothermolysis, the TRT of the average hair follicle lies between 10 and 100 milliseconds (ms). By choosing long pulses of light for hair removal, the risk of collateral skin damage to epidermal melanin is reduced.
Early q-switched lasers produced only a temporary hair-reduction effect as the laser pulses were far too short to damage the hair regrowth stem cells and terminal hair growth resumed immediately.
Effects on the hair follicle using laser and IPL for hair reduction
Thermal injury to human tissue has been established in computational and porcine studies to commence above 43.5°C and observable burn injuries to skin are evident from 50°C (Chandrasekhar, 1960; Wilson and Adam, 1983; Jacques and Prahl, 1987). However, the purpose of selective photothermolysis using laser and intense pulsed light sources, is to heat a specific chromophore found in the hair shaft to achieve thermal coagulation of the hair follicle and adjacent hair growth stem cells, without injuring perifollicular skin tissue. Computational studies show that the optimal temperature to selectively damage the hair shaft is 70°C for 1 ms; however, much longer pulse durations are required to allow heat to damage the adjacent follicular tissue containing the stem cells that initiate hair regrowth. The photothermal effect in hair reduction is infundibular dilation, plugging of keratin and clumping of melanin with disintegration and/or retraction of the intraluminal hair shaft as shown in the stained sections in Figure 4.
It is known that permanent hair reduction using laser or IPL specifically targets the melanin (pigment) in the follicle and that the hair follicle and its adjoining anatomical parts including the germ cells responsible for hair regrowth are effectively coagulated by laser or IPL thermal injury. However, the precise mechanism of hair growth delay and occasional recurrence of finer lighter hair is not fully understood.
Variations in light energy by skin and hair type—hair reduction
When lasers for hair reduction were first introduced there was a very limited choice between ruby lasers with sub-millisecond pulses and q-switched Nd:YAG lasers, both with small spot sizes on tissue. The ruby laser was slow and the 694 nm wavelength was only suitable for Fitzpatrick skin types 1–3, the sub-millisecond pulses and high energy did not give sufficiently long pulse durations to adequately heat the entire follicle and damage the surrounding hair regrowth stem cells. The nanosecond pulses of the Nd:YAG could be used on dark skin types but the effect of high peak power pulses only delivered ‘photo-waxing’ of the hair and hair regrowth patterns were similar to wax epilation.
The high energies used and small spot sizes of the ruby laser frequently led to overtreatment, especially in darker skin types (Bjerring et al, 1998).
Today, operators have a choice of wavelengths: ruby 694 nm; alexandrite 755 nm; diode 810 and 940 nm; long-pulse Nd:YAG 1064 nm; and broadband intense pulsed light (IPL). A wide range of pulse durations from nanoseconds for temporary hair reduction effects to several hundred milliseconds and large spot sizes with fast repetition rates for large area treatments is available.
In general, Fitzpatrick skin types 1–3 do best with alexandrite or diode laser and IPL, while darker skin types respond well to long-pulse diode and Nd:YAG laser. Modern IPL with narrow band-pass filters and time-resolved spectral outputs can be used successfully up to skin type 5. Thermoelectric (Peltier) parallel skin cooling, forced chilled air, cryogen spray and cooling gel packs have further simplified side-effect-free treatment.
The key to hair-reduction success is the need for contrast between hair and skin colour. Even where skin is naturally dark, providing the target hair is dark coarse hair then light-based epilation can be successful. However, usually lower energy density (fluence) is used and more treatments are required due to hair density and thickness.
Treatment time scales and evaluating the efficacy of the treatment
As explained earlier, hair grows in a cycle of three phases. Anagen phase is the growth phase of the hair. The catagen phase is a brief portion of the hair growth cycle in which the growth stops. The telogen phase is the dormant phase of the hair. Published studies indicate that hair can only be treated successful during the anagen phase. However, hair in various body areas grows at different rates and can vary in follicular density, colour and degree of coarseness.
Hairs are not all in the same growth phase at the same time as human hair grows asynchronously. This is why several treatments are needed. An average of 6–10 sessions is needed for hair-reduction treatment (more in dark skin types) in order to treat the whole area (depending on the hair colour, thickness, density, etc.). The normal gap between sessions, depending on the new growth cycle and the body area, is 4–10 weeks.
Any delayed partial regrowth following laser or IPL treatment may be thinner and/or lighter than the original hair that was treated. Hair miniaturisation is frequently observed. Clients should not expect full permanent clearance as typically an average of 75–85% clearance is achieved with very high patient-satisfaction rates.
Paradoxical hair growth
In some patients, optical hair removal treatment has a reported paradoxical effect of stimulating hair growth in 0.6–10% of patients (Moreno-Arias et al, 2002; Kontoes et al, 2006). This new terminal hair growth has been observed in areas untreated, but in close proximity to those treated is believed to involve the reactivation of dormant hair follicles. It is most often seen in middle-aged women of Mediterranean or South Asian origin (skin types 3–6) with an elevated body mass index (BMI) and is usually associated with polycystic ovarian syndrome (PCOS) and ovarian hyperandrogenism. In most cases, this paradoxical hair growth occurs at a site that has a high vellus count and is relatively free of terminal hairs, such as adjacent to untreated facial areas or neck and takes the form of fine, dark hair.
All laser and light sources have the potential to cause hair induction, but no clear relationship has been established between the types of hair removal device or the fluence used and the incidence of paradoxical hair growth (Alajlan et al, 2005). Possible causes include the effect of inflammatory mediators and subtherapeutic thermal injury causing induction of the hair cycle (Town and Bjerring, 2016).
When this unusual condition is seen, treatment with laser or IPL should be stopped for 6 months and some other form of hair removal such as waxing, threading or depilatory creams used before restarting the light-based treatment method.
Conclusion
Laser and intense pulsed light hair reduction are well-established treatment options for the removal of unwanted body and facial hair. Advances in technology and our understanding of the hair miniaturisation process following multiple exposures to laser and IPL energy have established this modality as one of the best alternatives for cosmetic hair reduction and long-term hair growth delay.