

Europe has seen a resurgence in the popularity of tattooing. Recent estimates show that approximately 10–20% of the general population in Europe are tattooed (De Cuyper and Pérez-Cotapos, 2018). Tattoo removal attempts date back to ancient Egypt, with numerous techniques having been used to remove unwanted tattoos, many of which cause damage to surrounding skin structures, often resulting in scarring and incomplete removal of the tattoo itself (Armstrong et al, 2008). Presently, effective removal can be achieved using lasers. Multiple laser treatments may be necessary, depending on the size of the tattoo, depth of ink placement and the colour of the inks used. Some tattoos cannot be entirely removed with lasers.
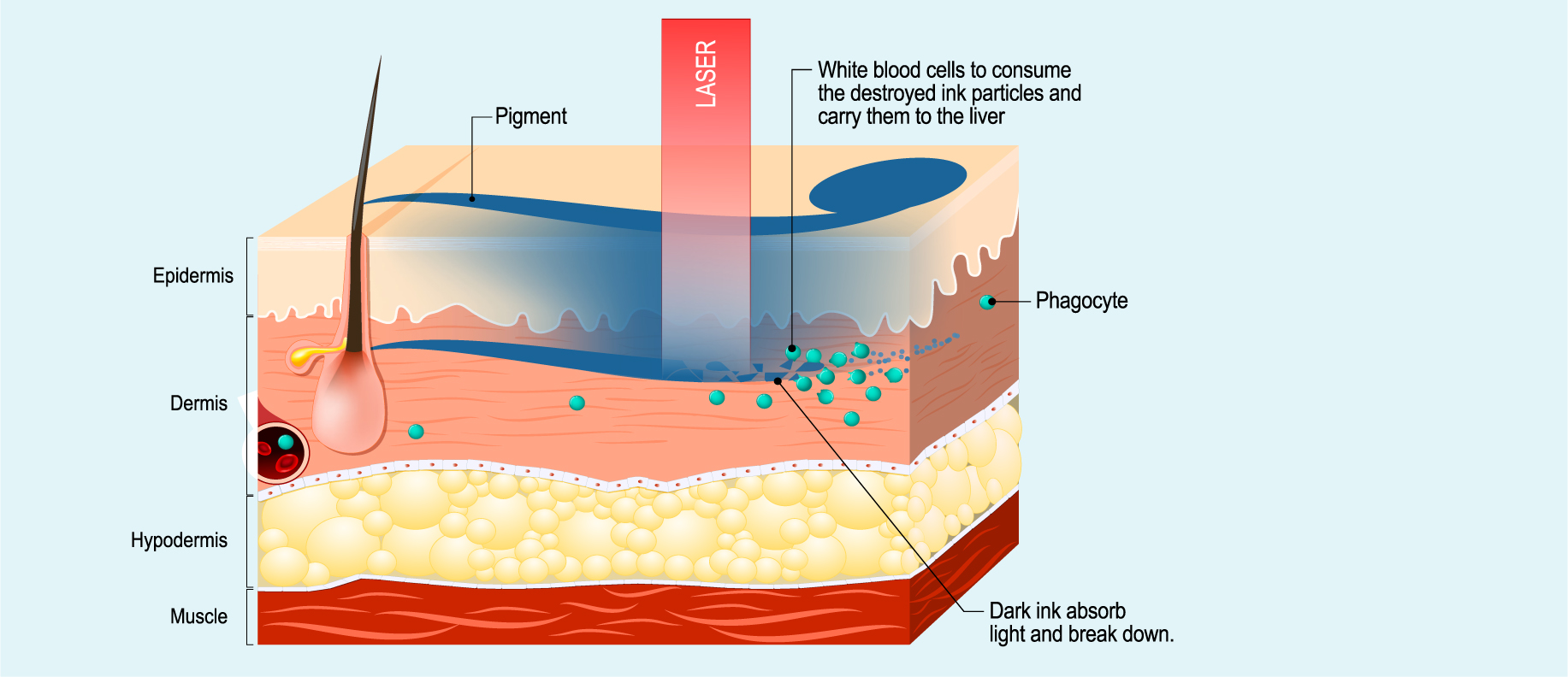
The laser selectively heats up and fragments the tattoo particles and the smaller pieces are then removed by normal bodily processes (Tay and Chan, 2011).
Box 1 gives definitions for some commonly used terms in laser tattoo removal.
| Chromophore | Part of a molecule that gives it its colour |
| Laser | A device that emits light through a process of optical amplification based on the stimulated emission of electromagnetic radiation |
| Wavelength | The distance between successive crests of a wave, especially points in a sound wave or electromagnetic wave |
| Photothermolysis | A precise microsurgery technique used to target tissue in a specific area. The specific wavelength of the laser is matched to the absorbance of the chromophore, which is heated and destroyed without affecting or damaging surrounding tissue |
Reasons for tattoo removal
Although the popularity of tattoos is on the rise, many people desire tattoo removal and, often, they are in a hurry to do so for various personal, social or occupational reasons (Aurangabadkar, 2015). Nouri (2018) states that approximately 28% of people regret their tattoo within the first month, and the most popular reason for tattoo removal is to ‘further enhance self-esteem by freeing oneself from the stigmatizing lesion that was the source of many years of regret’ (Nouri, 2018). Some may simply dislike the design or the position of their tattoo, and others may just want a new design in place of the original. There can be psychological reasons behind the desire for tattoo removal (e.g. removing an ex-partner's name). There can also be sociological reasons, for example, when an individual belongs to a particular professional field where visible tattoos are not acceptable.
Tattoo placement in the skin
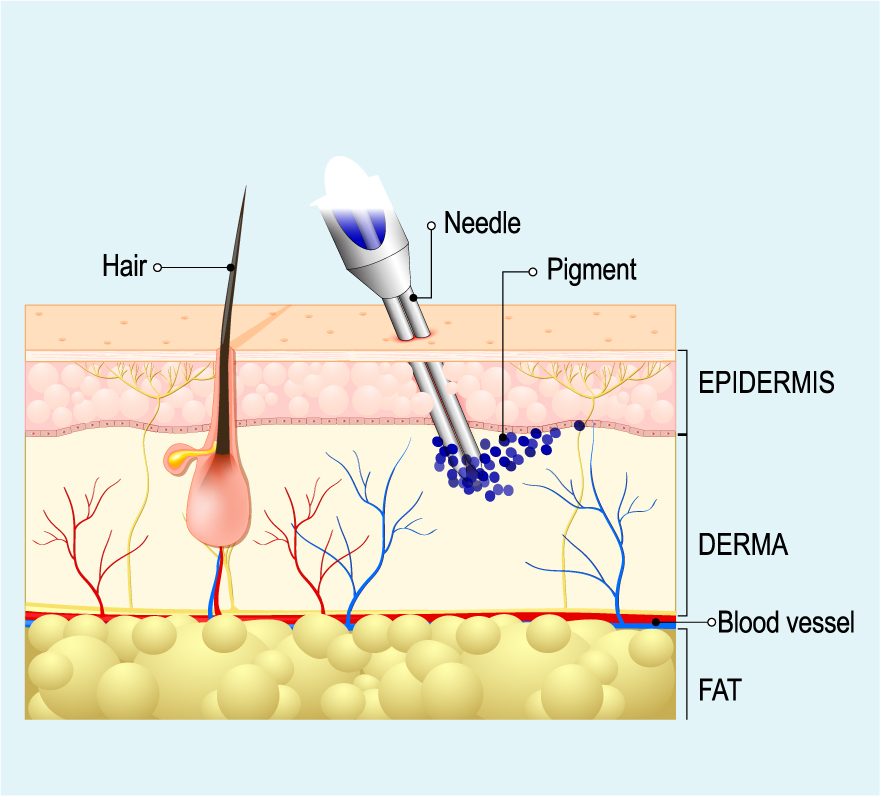
Tattoo ink particles are introduced, via a needle, into the upper to mid layer of the dermis, and remain visible through the uppermost epidermal layer (Figure 1, Box 2). Throughout the professional tattooing process, needles are dipped into ink and an electronic tattoo device injects ink particles through the epidermis to below the dermal-epidermal junction (usually with a constant depth of around 1 mm). Due to the skin's natural growth cycle, the epidermis is continually shed, so for the tattoo to become a permanent part of the skin, it is essential that the ink particles reach the dermal layer (Nouri, 2018). It is also important to note that the ink should not be placed deeper than the dermis, as this may increase the probability of scarring or the tattoo simply blurring or rapidly fading.
| Professional | Designed to be permanent, these are applied with a tattoo gun into the deeper dermis layer (Ho and Goh, 2015). Over time, ink colours can fade due to pigment migration into the deeper dermis and to regional lymph nodes via lymphatics. This is why older tattoos can appear blurry, while black inks have blue-grey hues (Naga and Alster, 2017) |
| Amateur | Amateur tattoos are from handheld needles that inject ink into various depths of the skin. Generally, they have fewer ink particles and are superficially placed. These tattoos are usually easier to remove due to their superficial placement (Naga and Alster, 2017). |
| Cosmetic | Often called permanent makeup, cosmetic tattoos are increasingly popular and include permanent eyeliners and eyebrows. However, they can be difficult to remove as the inks often used contain pigments of red, brown, white or flesh colours (Ho and Goh, 2015) |
| Medicinal | Tattoos can also be used in medicine, ranging from corneal tattooing to medical alert tattoos, where they alert medical staff during emergency situations (Ho and Goh, 2015) |
| Traumatic | These result from deposits of foreign objects (e.g. metal or glass) penetrating the skin. They can be difficult to remove if deeply embedded and if a patient develops a skin injury, a traumatic tattoo can result |
Macrophages in the dermis recognise the large tattoo ink particles as foreign entities and attempt to remove the ink molecules. However, most of the dye is captured and remains in the dermis.
Different methods for removal
Excision
The process of tattoo excision involves the tattoo being surgically removed. Depending on the size and location of the tattoo, this method can be a single process and may be a more desirable method for multicoloured tattoos or the residual ink a laser may otherwise be unable to treat. The end result will most certainly be a surgical scar in the location of the previous tattoo site, as well as the risk of post-operative infection to the wound. However, there are limitations to this method, including the size of the tattoo to be excised, with smaller tattoos being easier to remove.
Dermabrasion
Dermabrasion uses a wire brush or fast spinning diamond fraise or over the tattoo site to abrade the skin. This method removes skin tissue to the depth of the papillary dermis and minimises scarring, but can leave residual tattoo ink. This method can require multiple treatment sessions to remove professional tattoos from the skin entirely, which will increase the likelihood of post-treatment scarring.
Laser tattoo removal
As dermabrasion, excision and other generally more destructive methods of removal can cause scarring or incompletely remove tattos, laser removal become the gold standard for tattoo removal. Lasers selectively destroy the tattoo pigment using photothermolysis (De Cuyper and Pérez-Cotapos, 2018).
Using lasers
There are three types of Q-switched lasers used for the removal of tatoos: the Nd:YAG, ruby, and alexandrite lasers. In Q-switching, the laser produces short, nanosecond-long pulses with a much higher peak power than would be produced by the same laser in a constant beam (Bernstein, 2007). It has the advantages of being more target-specific and, thus, there is less chance of damage to surrounding tissue (De Cuyper and Pérez-Cotapos, 2018).
Anderson and Parrish's principle of selective photothermolysis (1983) led the way for laser use in dermatology and, consequently, the removal of tattoos. The principle is that ‘if the used wavelength is well absorbed by the target and the pulse width is equal to or shorter than the target's thermal relaxation time, the heat generated will be confined to the target’ (De Cuyper and Pérez-Cotapos, 2018). In this case, the target chromophores are the tattoo ink particles.
Each chromatophore absorbs light of a particular wavelength. Along with the tattoo pigments, there are also endogenous chromophores such as melanin, haemoglobin, oxyhaemoglobin and water, each of which has unique absorption characteristics. It is important to find the correct wavelength to affect the tattoo pigments rather than endogenous chromophores.
Apart from the wavelength, there are other factors that are important to consider when using lasers. The laser must penetrate far enough through the epidermis to reach the tattoo pigment. Additionally, the pulse duration must be long enough to heat the pigment so that it fragments, but short enough so that surrounding tissues are not affected by the heat generated. According to Farkas et al (2013), ‘two basic principles are involved in light–tissue interaction: absorption and scatter. Absorption is critical in the targeted treatment effect. The higher the absorption and less scatter, the less energy will be required to heat the target to the desired temperature and to achieve the resultant effect’.
Length of treatment
The number of tattoo removal sessions required depends on the tattoo itself rather than on the laser The tattoo size, depth and ink density, its age and the types of inks used are all factors in the length of time removal will take. For amateur tattoos, which are typically not as deep as professional tattos, 5–10 sessions tend to be standard, while 15–20 are more common for professional tattoos, with up to 25 sessions in rare cases (Sardana et al, 2015).
The Fitzpatrick skin type of the patient can also affect treatment length. While effectively used on all skin types, Q-switched lasers may have difficulty with complete pigment removal on patients with lighter skin (i.e. Fitzpatrick types I and II). Furthermore, the complete removal of older tattoos may not be achievable due to the possibility of some dermal pigment penetrating too deep to be reached (Nouri, 2018).
New developments
While very effective, Q-switched laser treatments are also time-consuming and costly, with the number of treatment visits needed, spaced a month or more apart, before removal is complete (Figures 3–5). Compared with the billionth of a second pulsed by Q-switched lasers, picosecond lasers pulse at a trillionth of a second (Smith, 2013).



By delivering the energy in a shorter period of time, picosecond lasers require less energy to clear pigment, and the damage to surrounding tissue may be minimised, says Dr Saedi, an investigator on one recent non-randomised clinical trial that enrolled 15 patients with dark tattoos. Using a picosecond laser, the investigators produced tattoo clearance of 75% or more in an average of 4.25 sessions, or about half the time associated with Q-switched lasers (Smith, 2013).
Post-laser tattoo removal
As with most procedures, for a desirable cosmetic result, post-procedure care is necessary when performing laser tattoo removal. A non-adhesive sterile dressing with aloe vera, placed over the tattoo site using surgical tape to keep the dressing in place, is ideal for post-laser treatment. The dressing should remain in place until the following day. Patients should not engage in physical exercise post-laser treatment or have a hot bath, while wearing loose clothing over the tattoo site is advisable. The tattoo site must remain clean and kept cool in the first instance by applying cooling aloe vera initially, and then using an intensive repair cream, such as a copper-based intense aqueous moisturiser, to help heal the site. Patients should expect some crusting and scabbing that could last approximately for 7–10 days post-treatment. Furthermore, patients may develop blisters to their tattoo site after their laser treatment, but these must not be burst due to the possible risk of infection. Ideally, the treatment site must not be sun exposed and a sun block must be applied daily.
Common side effects of laser tattoo removal
Hyperpigmentation
Yates et al (2010) state that hyperpigmentation could be a result of increased melanin production from the melanocytes as a response to laser-generated heat. Fading time of hyperpigmentation varies greatly amongst Fitzpatrick types and can occur in all skin types at any point in the course of laser tattoo removal. The chance of hyperpigmentation occurring is mainly due to skin type, with darker skinned patients (i.e. Fitzpatrick type III or IV skin) being higher risk. Measurements to be taken in the sun should be highlighted and emphasised to patients. Melanin in the epidermis can compete for the absorption of laser light intended for tattoo removal, which can cause destruction of the cells containing melanin. This can then lead to dyspigmentation, blistering or even scarring (Ho and Goh, 2015).
Hypopigmentation
A common side effect of laser tattoo removal is hypopigmentation, and the risk is higher with patients of darker skin types who undergo treatment using the Q-switched lasers. This risk also increases for all patients with the number of treatment sessions. Pfirrmann et al (2007) found that 38% of patients treated with Q-switched lasers experience hypopigmentation, which generally lasts for 2–6 months.
Scarring
Mariwalla and Dover (2006) state that the risk for scarring during laser tattoo removal is ‘highest on the chest, outer upper arm, and ankle’. Scarring risk is also increased, not just by the location of the tattoo, but also by the density of the pigment. Double tattoos, where one a tattoo covers an original tattoo, will have high-density pigmentation and increased resistance to the laser (Yates et al, 2010). Before treatment, patients should be asked about the possibility of a cover-up tattoo, as this may not be immediately obvious upon an initial inspection (Yates et al, 2010).
Blistering, bleeding and crusting
Blistering is a side effect that can occur after an overly aggressive laser treatment. The risk of this can be decreased with a tissue-cooling system (e.g. cryogen spray or contact chill tip) (De Cuyper and Pérez-Cotapos, 2018). It is important to ensure that treatments have intervals of at least 4 weeks to avoid blisters, wheals, punctate bleeding and crusts (Armstrong et al, 2008).
Resistant and residual ink
At times, it is difficult to completely remove a tattoo, in particular, multicoloured professional tattoos, and residual pigment or a faint image may remain even after numerous laser treatments (Khunger et al, 2015). It is thought that this is a result of the chemical make-up of the ink used, as well as the colour/size of the ink particles. Currently, there is no regulation governing the chemicals found within inks, so each tattoo can vary greatly in its chemical composition, which adds to the difficulties faced when attempting complete removal. In 2016, the European Commission began drafting EU-wide legislation for tattoo ink ingredients, with Karsai et al (2016) stating that the ‘number of pigments used in tattoos will possibly be reduced due to regulations on carcinogenic, mutagenic or toxic substances’. The result of laser tattoo removal is ‘dependent on both the size and the colour of the tattoo pigment’ (Sardana et al 2015). Residual ink can also be due to the fact that some colours are simply harder to break down than others, with Ho and Goh (2015) stating that the ‘QS ruby, alexandrite and Nd:YAG lasers are established technologies against blue, black, red and green tattoos, with varying degrees of effectiveness’. Tattoos of other colours can be found challenging to remove effectively.
Darkening cosmetic tattoos
Designed to match natural skin pigments that are tan, brown, black or red, cosmetic tattoos treated with the Q-switched laser can turn black or grey immediately after laser tattoo removal treatment. White tattoo pigment containing zinc or titanium oxides can also turn black post-treatment. Determining whether a tattoo contains white tattoo pigment at all, or how much it contains, can be difficult as various shades are produced by mixing white with other colours. After cosmetic or white tattoos turn grey or black, they can be removed with further laser treatment. However, it does typically take more treatments to remove these than when removing black tattoos (Bernstein, 2007).
Conclusion
In summary, there may be many reasons why a person may want to remove their tattoo. Laser removal is reasonable effective; however, complete removal is not always possible for a variety of reasons. Advances in laser technology have allowed a precise targeting of ink particles, thus minimising damage to adjacent tissues and reducing the chance of known side effects. With increased knowledge of the ink composition and further advances in laser technology, tattoo removal will only progress further with time.